
Success and Complication Rates of Transvenous Lead Extraction in a Developing High-Volume Extraction Center: The Zurich Experience
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
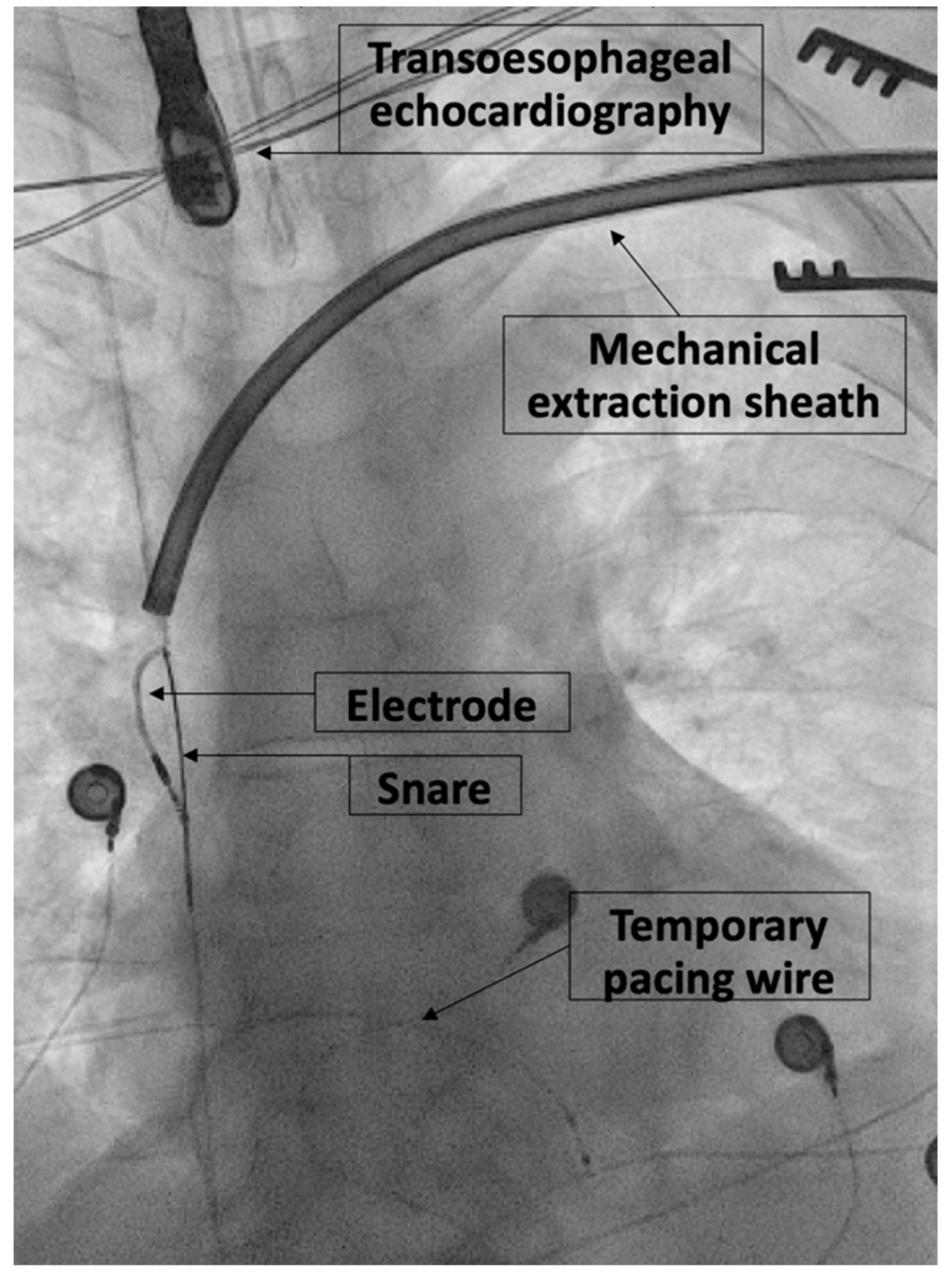
2.2. Extraction Procedure
2.3. Data Collection and Analysis
2.4. Definitions
3. Results
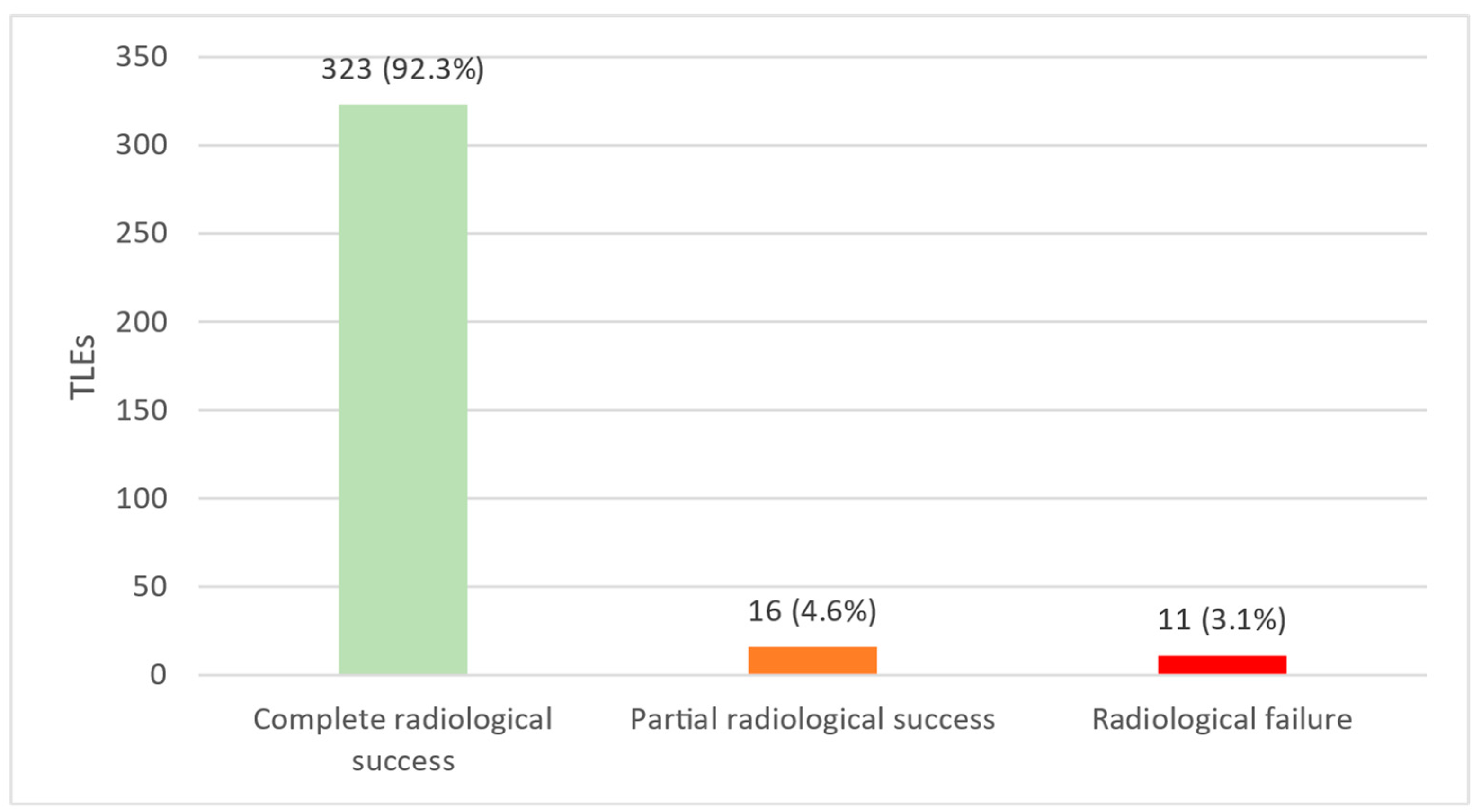
3.1. Radiological and Clinical Success
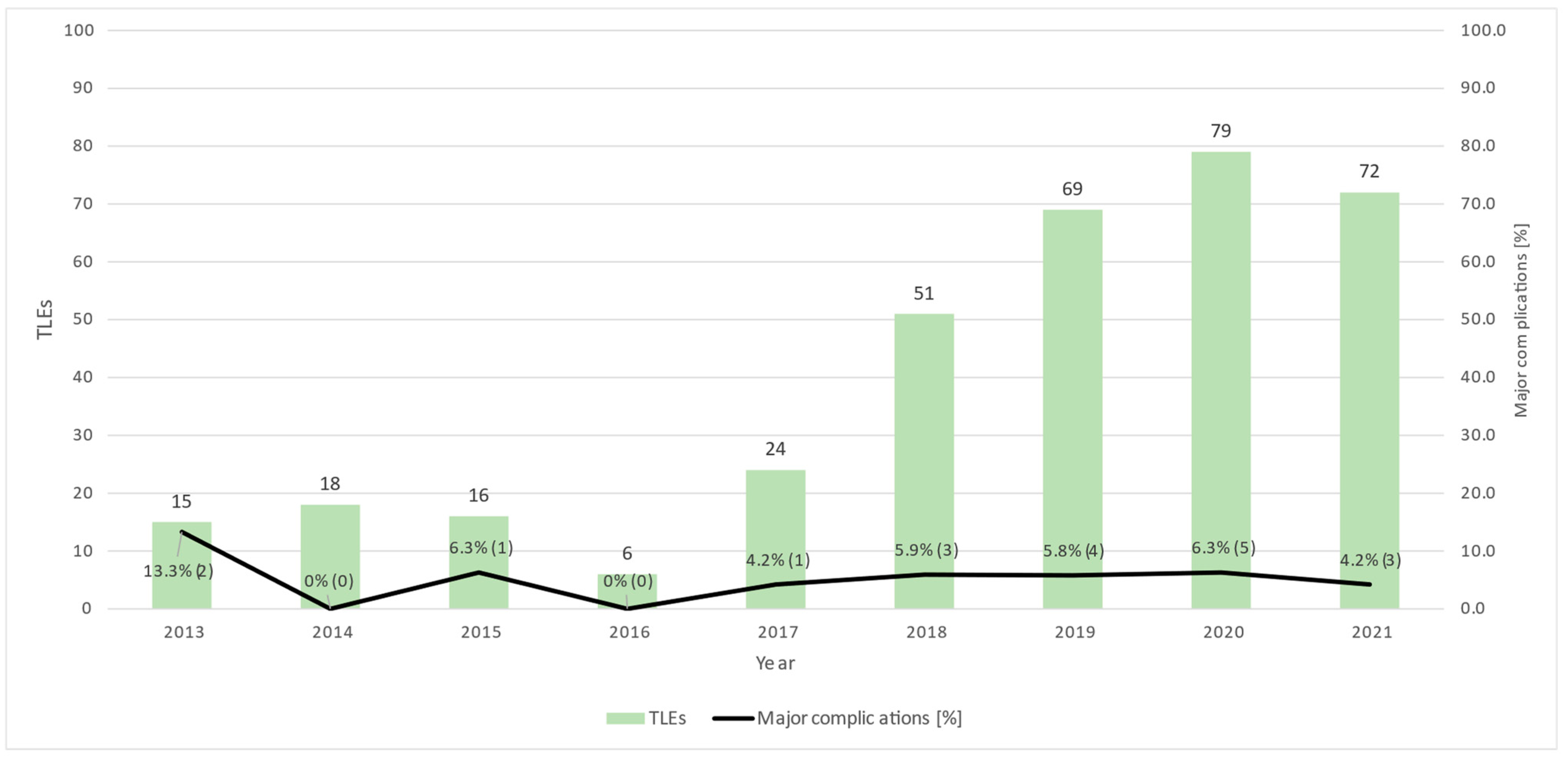
3.2. Complications
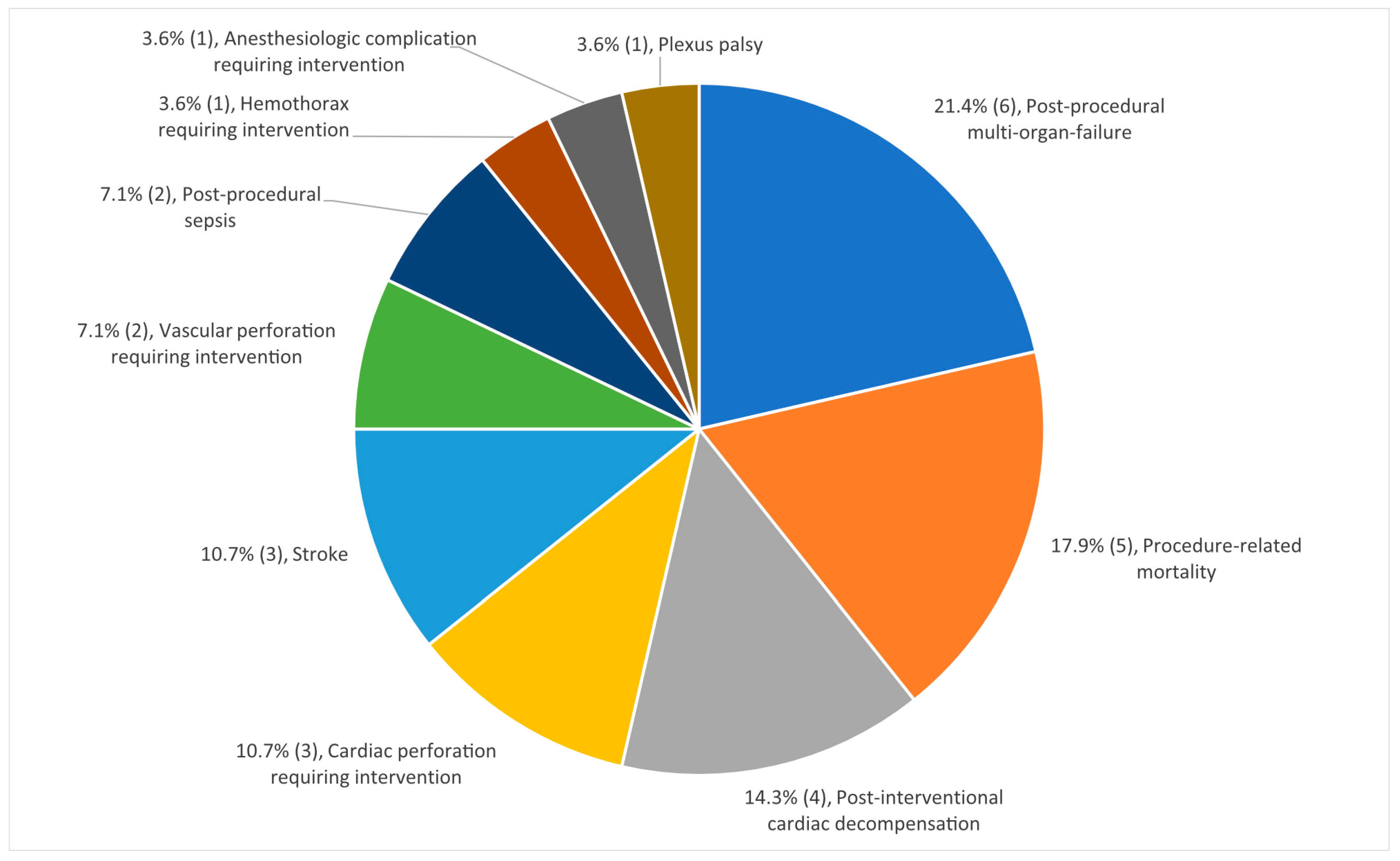
3.3. Major Complications
3.4. Procedure-Related Mortality
3.5. Minor Complications
4. Discussion
5. Conclusions
6. Limitations of This Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TLE | Transvenous lead extraction |
| CIED | Cardiac implantable electronic device |
| ICD | Implantable cardioverter–defibrillator |
References
- Diemberger, I.; Biffi, M.; Martignani, C.; Boriani, G. From lead management to implanted patient management: Indications to lead extraction in pacemaker and cardioverter-defibrillator systems. Expert Rev. Med. Devices 2011, 8, 235–255. Available online: https://pubmed.ncbi.nlm.nih.gov/21381913/ (accessed on 27 February 2023). [PubMed]
- Bongiorni, M.G.; di Cori, A.; Segreti, L.; Zucchelli, G.; Viani, S.; Paperini, L.; Menichetti, F.; Coluccia, G.; Soldati, E. Where is the future of cardiac lead extraction heading? Expert Rev Cardiovasc. 2016, 14, 1197–1203. Available online: https://pubmed.ncbi.nlm.nih.gov/27494362/ (accessed on 27 February 2023).
- Hauser, R.G.; Katsiyiannis, W.T.; Gornick, C.C.; Almquist, A.K.; Kallinen, L.M. Deaths and cardiovascular injuries due to device-assisted implantable cardioverter-defibrillator and pacemaker lead extraction. Europace 2010, 12, 395–401. Available online: https://pubmed.ncbi.nlm.nih.gov/19946113/ (accessed on 27 February 2023). [CrossRef] [PubMed]
- Kurtz, S.M.; Ochoa, J.A.; Lau, E.; Shkolnikov, Y.; Pavri, B.B.; Frisch, D.; Greenspon, A.J. Implantation trends and patient profiles for pacemakers and implantable cardioverter defibrillators in the United States: 1993–2006. Pacing Clin. Electrophysiol. 2010, 33, 705–711. Available online: https://pubmed.ncbi.nlm.nih.gov/20059714/ (accessed on 27 February 2023). [CrossRef] [PubMed]
- Wazni, O.; Epstein, L.M.; Carrillo, R.G.; Love, C.; Adler, S.W.; Riggio, D.W.; Shahzad, S.K.; Bashir, J.; Greenspon, A.J.; DiMarco, J.P.; et al. Lead extraction in the contemporary setting: The LExICon study: An observational retrospective study of consecutive laser lead extractions. J. Am. Coll. Cardiol. 2010, 55, 579–586. Available online: https://pubmed.ncbi.nlm.nih.gov/20152562/ (accessed on 27 February 2023). [CrossRef] [Green Version]
- Kennergren, C.; Bjurman, C.; Wiklund, R.; Gäbel, J. A single-centre experience of over one thousand lead extractions. Europace 2009, 11, 612. [Google Scholar] [PubMed]
- Bongiorni, M.G.; Kennergren, C.; Butter, C.; Deharo, J.C.; Kutarski, A.; Rinaldi, C.A.; Romano, S.L.; Maggioni, A.P.; Andarala, M.; Auricchio, A.; et al. The European Lead Extraction ConTRolled (ELECTRa) study: A European Heart Rhythm Association (EHRA) Registry of Transvenous Lead Extraction Outcomes. Eur. Heart J. 2017, 38, 2995–3005. Available online: https://pubmed.ncbi.nlm.nih.gov/28369414/ (accessed on 27 February 2023).
- Byrd, C.L.; Wilkoff, B.L.; Love, C.J.; Sellers, T.D.; Reiser, C. Clinical study of the laser sheath for lead extraction: The total experience in the United States. Pacing Clin. Electrophysiol. 2002, 25, 804–808. Available online: https://pubmed.ncbi.nlm.nih.gov/12049372/ (accessed on 27 February 2023).
- Sood, N.; Martin, D.T.; Lampert, R.; Curtis, J.P.; Parzynski, C.; Clancy, J. Incidence and Predictors of Perioperative Complications with Transvenous Lead Extractions: Real-World Experience with National Cardiovascular Data Registry. Circ. Arrhythm Electrophysiol. 2018, 11. Available online: https://pubmed.ncbi.nlm.nih.gov/29453324/ (accessed on 27 February 2023).
- Maytin, M.; Epstein, L.M. The challenges of transvenous lead extraction. Heart 2011, 97, 425–434. Available online: https://pubmed.ncbi.nlm.nih.gov/21296786/ (accessed on 27 February 2023). [CrossRef]
- di Monaco, A.; Pelargonio, G.; Narducci, M.L.; Manzoli, L.; Boccia, S.; Flacco, M.E.; Capasso, L.; Barone, L.; Perna, F.; Bencardino, G.; et al. Safety of transvenous lead extraction according to centre volume: A systematic review and meta-analysis. Europace 2014, 16, 1496–1507. Available online: https://pubmed.ncbi.nlm.nih.gov/24965015/ (accessed on 27 February 2023). [PubMed]
- Wilkoff, B.L.; Love, C.J.; Byrd, C.L.; Bongiorni, M.G.; Carrillo, R.G.; Crossley III, G.H.; Epstein, L.M.; Friedman, R.A.; Kennergren, C.E.H.; Mitkowski, P.; et al. Transvenous lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient management: This document was endorsed by the American Heart Association (AHA). Heart Rhythm. 2009, 6, 1085–1104. Available online: https://pubmed.ncbi.nlm.nih.gov/19560098/ (accessed on 27 February 2023). [CrossRef] [PubMed]
- Bongiorni, M.G.; Burri, H.; Deharo, J.C.; Starck, C.; Kennergren, C.; Saghy, L.; Rao, A.; Tascini, C.; Lever, N.; Kutarski, A.; et al. 2018 EHRA expert consensus statement on lead extraction: Recommendations on definitions, endpoints, research trial design, and data collection requirements for clinical scientific studies and registries: Endorsed by APHRS/HRS/LAHRS. Europace 2018, 20, 1217. Available online: https://pubmed.ncbi.nlm.nih.gov/29566158/ (accessed on 27 February 2023). [PubMed]
- Kusumoto, F.M.; Schoenfeld, M.H.; Wilkoff, B.L.; Berul, C.I.; Birgersdotter-Green, U.M.; Carrillo, R.; Cha, Y.-M.; Clancy, J.; Deharo, J.-C.; Ellenbogen, K.A.; et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm 2017, 14, e503–e551. Available online: https://pubmed.ncbi.nlm.nih.gov/28919379/ (accessed on 27 February 2023). [CrossRef] [PubMed] [Green Version]
- Starck, C.T.; Gonzalez, E.; Al-Razzo, O.; Mazzone, P.; Delnoy, P.P.; Breitenstein, A.; Steffel, J.; Eulert-Grehn, J.; Lanmüller, P.; Melillo, F.; et al. Results of the Patient-Related Outcomes of Mechanical lead Extraction Techniques (PROMET) study: A multicentre retrospective study on advanced mechanical lead extraction techniques. EP Europace 2020, 22, 1103–1110. Available online: https://academic.oup.com/europace/article/22/7/1103/5843500 (accessed on 28 February 2023). [CrossRef] [PubMed]
- Migliore, F.; Pittorru, R.; Dall’Aglio, P.B.; de Lazzari, M.; Rovaris, G.; Piazzi, E.; Dentico, A.; Ferrieri, A.; D’Angelo, G.; Marzi, A.; et al. Outcomes of transvenous lead extraction of very old leads using bidirectional rotational mechanical sheaths: Results of a multicentre study. J. Cardiovasc. Electrophysiol. 2022. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/jce.15767 (accessed on 28 February 2023). [CrossRef]
- Sharma, S.; Lee, B.K.; Garg, A.; Peyton, R.; Schuler, B.T.; Mason, P.; Delnoy, P.P.; Gallagher, M.M.; Hariharan, R.; Schaerf, R.; et al. Performance and outcomes of transvenous rotational lead extraction: Results from a prospective, monitored, international clinical study. Heart Rhythm. O2 2021, 2, 113–121. Available online: https://pubmed.ncbi.nlm.nih.gov/34113913/ (accessed on 28 February 2023). [CrossRef]
- Jones IV, S.O.; Eckart, R.E.; Albert, C.M.; Epstein, L.M. Large, single-center, single-operator experience with transvenous lead extraction: Outcomes and changing indications. Heart Rhythm 2008, 5, 520–525. Available online: https://pubmed.ncbi.nlm.nih.gov/18325849/ (accessed on 27 February 2023). [CrossRef]
- Bongiorni, M.G.; Soldati, E.; Zucchelli, G.; di Cori, A.; Segreti, L.; de Lucia, R.; Solarino, G.; Balbarini, A.; Marzilli, M.; Mariani, M. Transvenous removal of pacing and implantable cardiac defibrillating leads using single sheath mechanical dilatation and multiple venous approaches: High success rate and safety in more than 2000 leads. Eur. Heart J. 2008, 29, 2886–2893. Available online: https://pubmed.ncbi.nlm.nih.gov/18948356/ (accessed on 27 February 2023). [CrossRef] [Green Version]
- Parkash, R.; Crystal, E.; Bashir, J.; Simpson, C.; Birnie, D.; Sterns, L.; Exner, D.; Thibault, B.; Connors, S.; Healey, J.S.; et al. Complications associated with revision of sprint fidelis leads: Report from the canadian heart rhythm society device advisory committee. Circulation 2010, 121, 2384–2387. Available online: https://www.ahajournals.org/doi/abs/10.1161/CIRCULATIONAHA.109.924357 (accessed on 27 February 2023).
- Sidhu, B.S.; Gould, J.; Bunce, C.; Elliott, M.; Mehta, V.; Kennergren, C.; Butter, C.; Deharo, J.-C.; Kutarski, A.; Maggioni, A.P.; et al. The effect of centre volume and procedure location on major complications and mortality from transvenous lead extraction: An ESC EHRA EORP European Lead Extraction ConTRolled ELECTRa registry subanalysis. EP Eur. 2020, 22, 1718–1728. Available online: https://academic.oup.com/europace/article/22/11/1718/5874070 (accessed on 1 March 2023). [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lead explantation | Removal of the lead by simple traction techniques and lead dwelling time below one year. |
| Lead extraction | Removal of at least one lead with a dwelling time of more than one year. |
| Complete radiological success | Removal of all targeted leads and material without any indwelling lead remaining. |
| Partial radiological success | Lead remnants <4 cm after TLE. |
| Radiological failure | Incapacity to remove lead, >4 cm of targeted lead remaining. |
| Clinical success | Achieving the clinical result for which the TLE was performed. Complete radiological success or partial radiological success, when the remaining lead fragment <4 cm, does not increase the risk of further complications, such as perforation, embolic events, conservation of infection, or any other undesired outcome. Absence of any procedure-related major complication resulting in permanent disability or death. |
| Clinical failure | Incapacity to achieve clinical success. |
| Major complications | All complications causing persistent or significant disability, life-threatening events or death, or necessitating surgical intervention to prevent the above. |
| Procedure-related major complications | Complications presumably related to TLE necessitating surgical intervention, requiring extension of hospitalization, causing persistent or notable disability, life-threatening events, or death. |
| Minor complications | Any undesired event occurring during the same hospital stay as TLE requiring medical intervention, observation, or minor procedural intervention without requiring extension of hospitalization, causing persistent or notable disability, life-threatening events, or death. |
| Reoperation | Surgical or interventional operation during the same hospital stay caused by a complication after TLE (procedure-related or unrelated). |
| Patients treated | 350 |
| Mean age (years) | 63.6 ± 15.3 |
| Male sex | 251 (71.7%) |
| LVEF < 50% | 168 (48.0%) |
| LVEF absolute (%) | 45.7 ± 15.1 |
| Hypertension | 202 (57.7%) |
| Diabetes | 73 (20.9%) |
| Renal insufficiency (eGFR < 60 mL/min) | 121 (34.6%) |
| Anticoagulants Single antiplatelet therapy Dual antiplatelet therapy Oral anticoagulation Oral anticoagulation and antiplatelet therapy None | 79 (22.6%) 6 (1.7%) 148 (42.3%) 16 (4.6%) 101 (28.9%) |
| Indication for TLE Lead dysfunction Infection Device upgrade Other | 176 (50.3%) 108 (30.9%) 37 (10.6%) 29 (8.3%) |
| Procedure average duration (min) | 131.7 ± 66.3 |
| Mean lead dwell time (months) | 112.5 ± 78.6 |
| Type of lead Passive fixation ICD leads Dual-coil ICD leads Right ventricular leads Right atrial leads Left ventricular leads (coronary sinus) | 115 (32.9%) 158 (45.1%) 76 (21.7%) 194 (55.4%) 243 (69.4%) 69 (19.7%). |
| Mean number of leads extracted Extracted leads per patient 1 2 3 4 5 | 1.9 ± 0.8 117 (33.4%) 165 (47.1%) 51 (14.6%) 12 (3.4%) 2 (0.6%) |
| Device reimplantation | 263 (75.1%) |
| Type of Major Complication | Number of Affected Patients |
|---|---|
| Post-procedural multi-organ failure | 6 (1.7%) |
| Procedure-related mortality | 5 (1.4%) |
| Post-interventional cardiac decompensation | 4 (1.1%) |
| Cardiac perforation requiring intervention | 3 (0.9%) |
| Stroke | 3 (0.9%) |
| Vascular perforation requiring intervention | 2 (0.6%) |
| Post-procedural sepsis | 2 (0.6%) |
| Hemothorax requiring intervention | 1 (0.3%) |
| Anesthesiologic complication requiring intervention | 1 (0.3%) |
| Plexus palsy | 1 (0.3%) |
| Specific Mortality | Number of Affected Patients |
|---|---|
| Procedure-related mortality | 5 (1.4%) |
| In-hospital mortality | 11 (3.1%) |
| All-cause mortality within 30 days | 13 (3.7%) |
| Type of Minor Complication | Number of Affected Patients |
|---|---|
| Hematoma without need for intervention | 18 (5.1%) |
| Newly developed severe tricuspid regurgitation | 10 (2.9%) |
| Swelling of the arm/thrombosis | 10 (2.9%) |
| Pericardial effusion without need for intervention | 8 (2.3%) |
| Blood transfusion | 8 (2.3%) |
| Acute renal failure | 7 (2%) |
| Vascular complications with minor intervention | 6 (1.7%) |
| Hematoma with surgical revision | 5 (1.4%) |
| Electrode dislocation requiring revision | 4 (1.1%) |
| Pneumothorax requiring drainage | 2 (0.6%) |
| Pulmonary embolism | 2 (0.6%) |
| Anesthesiologic complication | 2 (0.6%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hofer, D.; Kuster, N.; Bebié, M.C.; Sasse, T.; Steffel, J.; Breitenstein, A. Success and Complication Rates of Transvenous Lead Extraction in a Developing High-Volume Extraction Center: The Zurich Experience. J. Clin. Med. 2023, 12, 2260. https://doi.org/10.3390/jcm12062260
Hofer D, Kuster N, Bebié MC, Sasse T, Steffel J, Breitenstein A. Success and Complication Rates of Transvenous Lead Extraction in a Developing High-Volume Extraction Center: The Zurich Experience. Journal of Clinical Medicine. 2023; 12(6):2260. https://doi.org/10.3390/jcm12062260
Chicago/Turabian StyleHofer, Daniel, Noah Kuster, Michelle C. Bebié, Tom Sasse, Jan Steffel, and Alexander Breitenstein. 2023. "Success and Complication Rates of Transvenous Lead Extraction in a Developing High-Volume Extraction Center: The Zurich Experience" Journal of Clinical Medicine 12, no. 6: 2260. https://doi.org/10.3390/jcm12062260